Knee Injuries and OA
Introduction
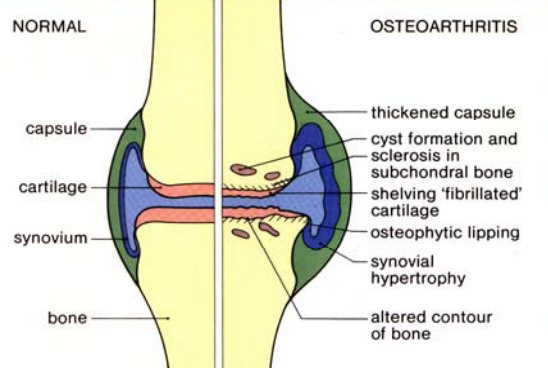
Osteoarthritis
Harris: Kelley’s Textbook of Rheumatology, 7th ed.
“Osteoarthritis (OA) is a degenerative joint disease, occurring primarily in older persons, characterized by erosion of the articular cartilage, hypertrophy of bone at the margins (i.e., osteophytes), subchondral sclerosis, and a range of biochemical and morphologic alterations of the synovial membrane and joint capsule. Pathologic changes in the late stages of OA include softening, ulceration, and focal disintegration of the articular cartilage; synovial inflammation also can occur.”
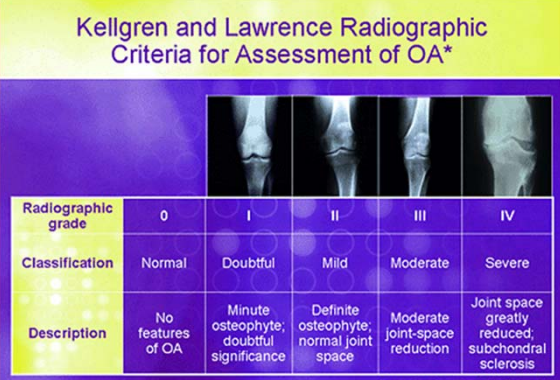
Kellgren and Lawrence Radiographic Criteria for Assessment of OA
OA Social and Economic Impact
- Osteoarthritis (OA) is the most prevalent form of arthritis in the elderly accounting for 34% of self-reported chronic pain (Breivik et al. 2006).
- Prediction of 8.5 million people in the UK had osteoarthritis (Arthritis Care, 2014)
- 1 in 8 days of restricted activity is due to osteoarthritis
- Each year 2 millions adults visit their GP because of OA
- The knee is the most common joint disorder with 13% of individuals over the age of
- 65, accounting for 97% of all primary knee replacements (Felson et al. 1998)
- In the UK alone, over 73545 patients had a form of total knee replacements for
- osteoarthritis in 2016 with an estimated economic burden of over £300 million
- 2.5% increase compared to 2008, and a predicted increase of 100% by 2030.
Effects of Knee OA on the Individual
- Pain
- Psychological Issues
- Physical Impairments
- Co-morbities
- Reduced function and lower quality of life
Osteoarthritis: Future Shock in U.K.
(GAD, 2006)
Aging of the population 2006 – 19% over 55 2025 - 25% over 55
Obesity a Strong Risk Factor for OA
Pain and Stiffness -> Disuse -> Weight Gain - Pain and Stifness…
Felson et. al. 1992
- 50% decrease in OA with 11% wt loss
- Larger effect in women
Does Running increase your risk of Knee OA?
Long distance running and knee OA: A Prospective Study Chakravarty et al (2008)
- 45 long-distance runners, 53 controls
- Middle aged adults, ave. 58
- Running minutes/wk: 214 vs 28
- Followed for 18 years (xrays, pain)
- No difference in joint space, pain score, or incidence/severity of OA
- Moderate running on normal joints is healthy
- However, if one has any knee injury, orthotic management needs to be thought about carefully
Running has significant benefits:
- Less obesity
- Less diabetes
- Less heart disease
- Less depression
- Better bone density
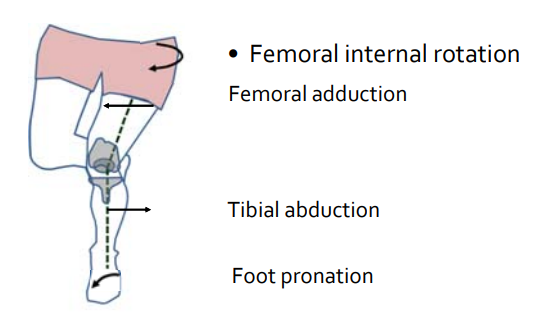
Knee Valgus
Understanding and Measuring Knee Valgus
In this work we are:
- Developing our understanding of the relationships between the presence of knee valgus angles & knee abduction moments and significant knee injury
Understanding and Examining Ways to Reduce Knee Valgus
Attempting to develop optimal management strategies to improve functional performance in relation to optimal limb alignment control
Characterisation of Risk Factors for Injury or Future Knee OA
Understand at-risk movements (cutting); and the role of knee surgery on future osteoarthritis progression
Patellofemoral Pain e (PFP)
- PFP is the most frequently diagnosed condition in patients with knee complaints
- Prevalence: 7%- 19% of the general population
- Majority of patients with PFP develop persistent complaints
Dynamic Knee Valgus
- Higher risk: ACL rupture & PFJ injuries
- Especially football,basketball, netball, handball
Rehabiitation of Neuro-muscular Control
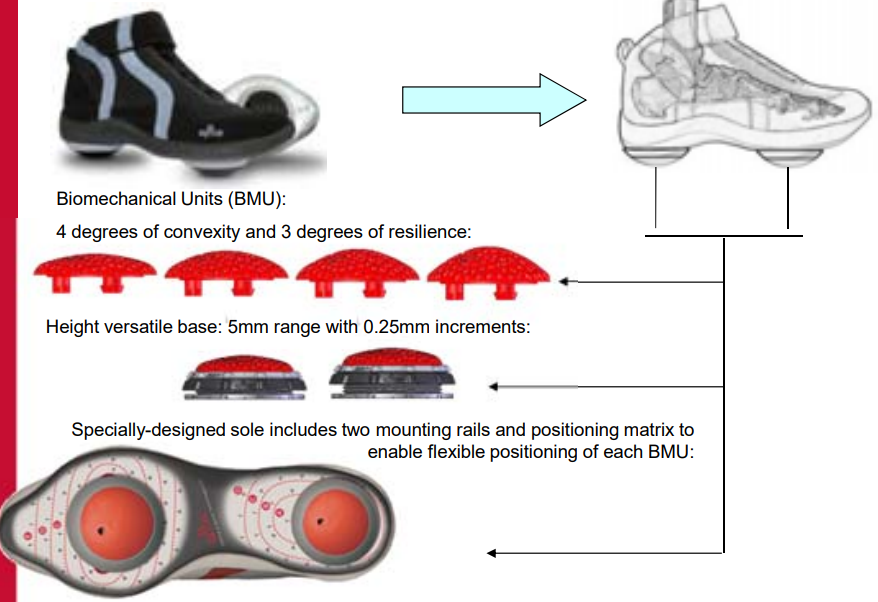
The AposTherapy System
Knee Injuries
- Knee injuries account for nearly 50% of all sports injuries
(Olsen et al., 2003).
- Anterior cruciate ligament injury is considered one of the most disabling severe knee injuries
(Lehmann et al., 2017).
- Approximately 200,000 ACL injuries in the US with an incidence of 84 per 100,000
(Bates et al., 2015).
- 81 per 100,000 in Sweden.
Frobell et al., (2007)
- 30 per 100,000 in UK.
Webb and Corry (2000)
Dynamic Knee Valgus
Overall annual rate of ACL injuries increased by 147.8% from 2.74 per 100,000 population in 2005⁄2006 to 6.79 per 100,000 in 2014⁄2015.
The majority (96.9%) of these injuries were in 10‐ to 14‐year‐olds
(Shaw and Finch (2017).
- Graft rupture in children and adolescents (6‐19 years) is 13% with the contralateral knee being 14% (Kay et al., 2018).
ACL Injuries
A significant debilitating injury leading to residual restriction of activity and mobility.
Season ending, career threatening (Myklebust et al., 2003; Lohmander et al., 2004).
Can occur in both contact and non‐contact in nature and occur in all types of sports, at all levels of play.
Sports involving planting, cutting and rapid decelerations
have the greater risk (Ireland, 1999; Olsen et al., 2004)
Incidence of ACL Injury in Sports
Football players over 50%, basketball players (10%), volleyball players (3%) and wrestling players (3%).
The lowest numbers for ice hockey and baseball players (1.16%)
Women sustain ACL injuries at higher rates than men in the comparable sports (2‐4 times greater).
Injury rate is higher in competition than practice.
Female Gender
- Hormonal Influences
- ACL has estrogen receptors
- Estrogen can cause ligament looseness
- Estrogen levels increase in girls compared to boys
- Estrogen increased at specific times in menstrual cycle
- Studies VERY inconsistent
- Every phase of cycle has been implicated in at least 1 study
Knee anatomy:
- Smaller intercondylar notch
- ACL may get stretched across bone and torn
- Athletes with bilateral ACL injuries have smaller ICN
Lower extremity alignment:
- Women more knock‐kneed
- May allow quad to exert more stress on ACL
- Data not exactly full scientific though
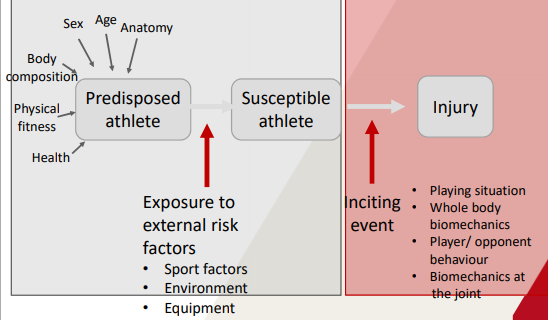
Risk Factors
Surgery vs No Surgery
- Surgery is better option for recovery
- Surgery leads to increased chance of OA