Lower limb Prosthetics
Prosthesis Structure
Structural Components
- Socket
- Suspension
- Container
- Joints -> hip, knee, ankle
- Connectors -> tubes between joints
- Floor interface -> foot, bung
- Additional mobility
Overall Structure
- Endoskeletal & Exoskeletal
- Cosmesis – constrainted movement unless 2-part

Statistics of the Referred Population
Service Centres in the UK
- England: 35
- Northern Ireland: 1
- Scotland: 5
- Wales: 3
2010⁄11 statistics from: www.limbless-statistics.org
Types of Data Collected
There are 2 classifications:
Primary
- Sex
- Site
- Side
Secondary
- Centre
- Years between Referral & Birth
- Weeks between Referral & Amputation
- Months between Amputation & Birth
- Ethnic Background
- Level of Amputation
- Cause of Amputation
Lower Limb Numbers
Overview
91% lower limb absence (very little movement analysis on upper limbs)
- 29% females
- 71% males
- 94% single sided
- 6% double sided
- 0.017% x-site, triple, quadruple
Cause
- 10% trauma
- 52% dysvascularity
- 9% infection
- 1% neurological disorder
- 3% neoplasia
- 5% congenital absence
- 20% no data
Level
- ~0% hemiplevectomy
- 3% hip disarticulation
- 37% trans-femoral
- 3% knee disarticulation
- 54% trans-tibial
- 1% ankle disarticulation
- 2% partial foot
- ~0% foot digits
- ~0% congenital absence
Ages(years)
- 3% ≥ 00 & ≤ 15
- 27% > 15 & ≤ 54
- 20% > 54 & ≤ 54
- 24% > 64 & ≤ 54
- 26% > 74
Disarticulations vs Through-bone
Advantages and Disadvantages of Disarticulations
Disarticulations – e.g. hip, knee, ankle
- distal (end) bearing
- less need for weight distribution
- less need for intrusive proximal socket extension
- self-suspending
- potentially greater range of motion
- potentially less space for distal components
- potentially segment length difference compared to sound side
Details on Main Prosthesis Components
Socket Shapes and Suspension
Trans Tibial
PTB Sockets Predominantly patella tendon bearing (PTB) sockets

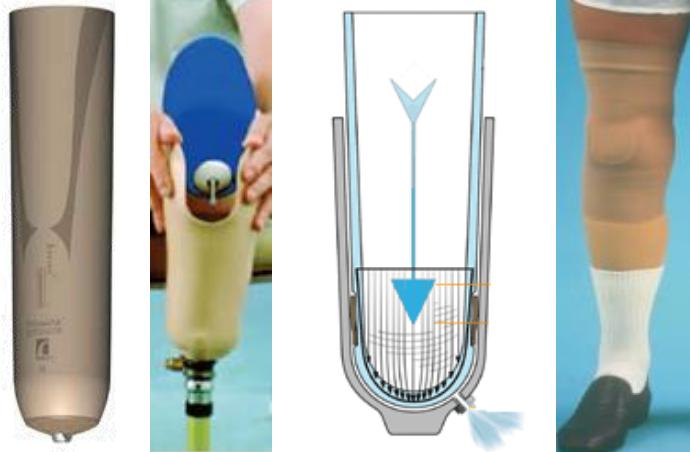
Total Contact Sockets With e.g. roll-on liners (pin, hypobaric (suction)), sleeves (suction)
No 8 (conventional plug fit) Thigh corset with articulated side-steels

Trans Femoral
MAS Very rarely Marlo Anatomical Socket (MAS)

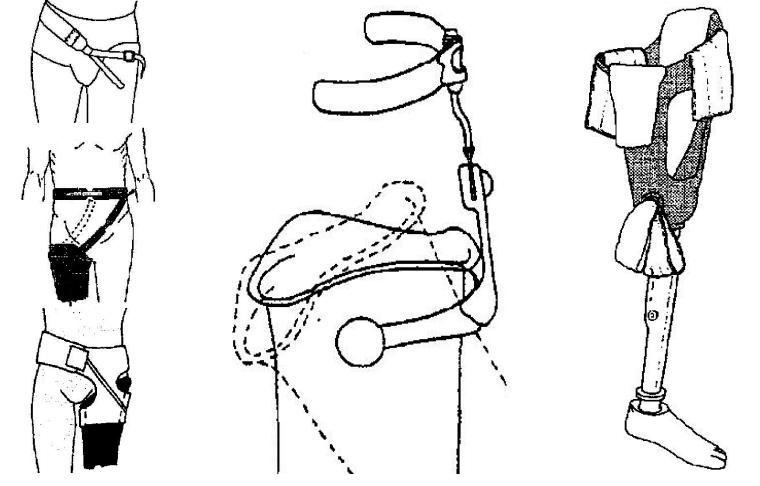
Suspension
- Soft suspension, pelvic band, suction, osseointegration
- Roll-on liners (pin, lanyard, hypobaric (suction)) – as shown before
Knees
Classifications
- No knee
- Mechanical -> mechanical, pneumatic, hydraulic friction
- Microprocessor -> pneumatic, hydraulic, magnetorheological friction
- Power -> motor assist
Overview of Function
Swing flexion – for swing phase AND sitting
- allows knee flexing
- single axis or polycentric rotation mechanism
Swing control – for swing phase
- controls rate of swing
- resistance, assistance
Stance control – for stance phase AND standing
- prevents knee flexing
- GRF anterior to knee, weight/user activated locking mechanism
Stance flexion – for stance phase
- flexes knee without collapsing
- rotation around secondary axis while primary axis is locked
Control in Microprocessor / Power Knees
- Real-time control
- Accommodation
- force – variable stiffness
- terrain – ROM in various positions
- speed – variable loading
- user specific motion – sitting & stair mode
- gait asymmetry – stance & swing
- Energy
- dissipation – correct time & angle
- return – correct time & angle
Martin J, Pollock A, Hettinger J. Microprocessor lower limb prosthetics: Review of current state of the art. Journal of Prosthetics and Orthotics. 2010;22(3):183-93.
Feet
Classifications
- Adapt to ground during stance
- Push off at late stance
- Ground clearance during swing
Overview of Function
- Passive feet
- non-energy storing & return (standard feet)
- energy storing & return (ESR) (or dynamic response)
- self-aligning feet (standard & ESR)
- Active feet
- passive power (for ground clearance)
- active power (for ground clearance & push off)
Design Features
- similar choice for all levels (except from long trans-tibial level downward)
- 1-3 axes (all planes)
- torque absorber & shock absorber
- removable cover
- adjustable heel height
- definition of toes (split toe option)
- colours (light / dark)
- exchangeable elastic elements (vary stiffness)
- separate ankle joint e.g. Blatchford Endolite Multiflex
- mechanism / electronics linked to knee e.g. Hydracadence, Symbionic leg
Additional Mobility
Overview
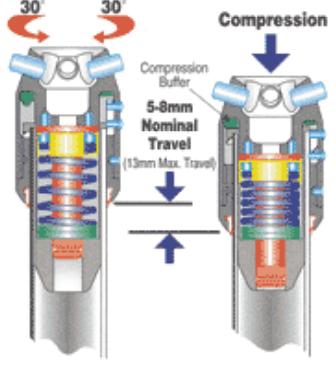
- Torque and/or shock absorber
- Rotators
Amputee Gait Analysis
Prosthesis Simulator
Help to recruit from typical healthy population instead of from limbless population for research purposes

Marker Location
- Segements are rigid & small surface area can be extended
- Take care with polycentric (instantaneous CoR) designs
- see Miller & Childress, May 2005, Robotica;23(03):329-35

Segment Properties
Prosthetic foot & shank (for trans-tibials) - Mass – scales (incl. water bag inside the socket for residuum mass - Lengths - ruler (in 3 directions) - CoM - knife edge - RoG - pendulum
Anatomic foot & shank (for trans-tibials) - Subtract prosthesis mass (incl. water bag) from body mass (incl. prosthesis) - to obtain body mass as if amputated through knee
- From anthropometric data, calculate body mass if not amputated
- to obtain more accurate anatomic segment mass
What is a prosthesis?
A prosthesis is a device that replaces a part of a body that was either absent from birth or has been lost due to injury, illness and / or deformity
First Major Improvements
1912 when an aluminium prosthetic leg was created by Marcel and Charles Desoutter after Marcel lost a leg in an aviation accident. The aluminium leg weight about 1.8 kg instead of the usual 3.5 to 4.5 kg at the time.
Lots of materials and techniques borrowed from the aviation industry.
1969 – Otto Bock invents the first modular prosthetic system, facilitating ease of changing components and alignment of the prosthesis
Conventional Prosthesis
Exoskeletal.
Most of these were still common in the UK in the late 1980’s

Modular Systems
Endoskeletal
Add/change components that give you available features for each joint being replaced
Adjustable – easier to change socket, length and alignment
Easier to make and repair if parts are available
Key Considerations
The ‘Fit’ (the prosthetic interface with the residual limb)
The Function-how useful it is
Biomechanics is central to comfort and function
The Cosmesis-its appearance
The Residuum
The residual limb has been described as an outer envelope of the skin and soft tissue surrounding a central strut, the skeletal shaft.
The soft tissue which covers the residuum is not designed for weightbearing
Trans-tibial has no horizontal weightbearing surface.
The qualities of the skin coverage and the amount and consistency of soft tissues is variable.
The difficulties with fluctuation
Differing amputation techniques – the quality of the residuum has a huge impact on rehabilitation!
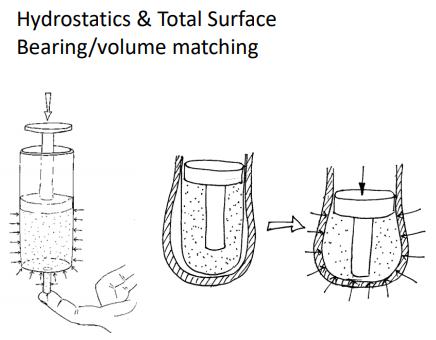
Weightbearing, Stability & Suspension
The socket has to stabilize bone structure in all planes of motion through soft tissue in a manner which is comfortable and causes no damage or detriment to the soft tissue.
The socket has to act as a mechanical junction or coupling between the soft tissue and skeleton of the residual limb and the rigid structure of the prosthesis during non-weight-bearing situations. The aim is to have minimum longitudinal displacement between weight bearing and non-weight bearing phases.
Weightbearing
Stability
If the bone structure is not stable then the socket will be able to move causing instability and there will be lessened control at joints
Suspension
Mechanical – Utilisation of a bony structure that they hook over such as the femoral condyles or iliac crests or radial compression and coefficient of friction
Suction – The creation of a situation where negative pressure creates a vacuum – Active vacuum
A Good Socket
“A Good fit is not Primarily defined by a particular shape of socket, but by the accommodation of the forces or pressures between the stump and socket to provide for comfortable and harmless weight-bearing, stabilisation and suspension.” Klasson B 1995
Cosmetics & Range of movement.
Revisiting theories/techniques as materials and technology changes
Redheads, R., (1979) - total surface bearing socket really came into play with ICEROSS and other liners
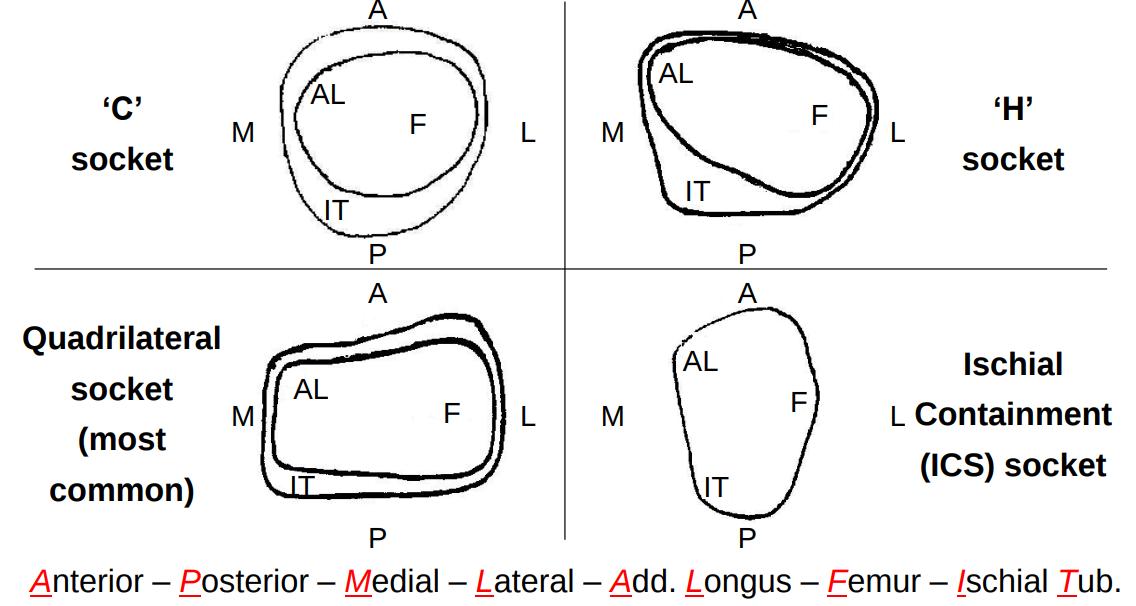
Names of Socket Types
Trans-femoral
- Quadrilateral
- ‘H’ for health
- ‘C’ for conventional
- Ischial containment sockets
- Marlo Anatomical socket
- Hifi
- Hybrid
- Ossur trans-femoral Socket
- Sub ischial sockets
Trans-tibial
- Patella tendon bearing
- Patella tendon bearing with
- supracondylar
- Patella tendon bearing with supracondylar and supra patella
- Total surface bearing
Evidence for which is the Best Socket?
Not enough and often small scale (extraneous variables)
Still many issues
ICS more comfortable than quadrilaterals (Hachisuka et al, 1999)
Or perhaps not (Boonstra et al.,1994)
MAS sockets have also been reported to improve gait efficiency, ease ascending slopes and sitting in soft chairs (Traballesi, et al, 2011) and provide greater ischial containment and medio-lateral stability than other sockets and that it also reduces trim lines which improves hip range of motion, (Trower, 2006; Perry, 1992; Flandry et al, 1989; Klotz, 2011).
Limited Hip flexion Hagberg (2005)
Osseo-integration
- No need for a socket
- Improved control of prosthesis
- Improved range of motion
- Increased sensation of external world.
- Risk of infection
- Still need to consider alignment
- Needs of surgery
- Need for the removal of the abutment
- Need for quality bone to implant into

Alignment
The relationship between the socket and the remaining elements of the prosthesis is key
The relationship between each joint in the lower limb is also key
Symmetry is often (but not always) sought
Primary (new) patients will often need a number of re-adjustments, to both socket and prosthetic componentry
These factors will influence prescription
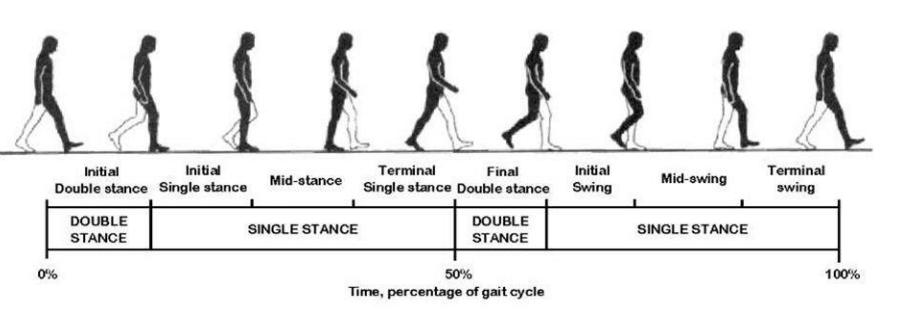
Gait Cycle
Energy Consumption and the Impact on Muscular Skeletal Structure.
- Is energy consumption as high as previously thought?
- Alignment
- Socket fit
- Level of amputation
- Componentry
Thermal discomfort.
Sweating
Environmental component – where you live
Increase risk of infection
Increase risk of tissue damage when the skin is damp
Individual differences in level of sweating
Decreased surface area increased sweating
Surrounded in an insulator
Solution - Assessment & Prescription
Finding out what is the best choice for the patient’s needs
Identifying the best generic component for the patient
Communicating the ideas for prescription to the patient
Identifying means of support, and discussing options and rehabilitation plans with other members of the MDT
Producing the first stage of the socket
Componentry
- Hips
- Knees
- Feet
- Torque Absorbers
- Shock absorbers
- Rotators
Hips
Types
2 types:
- Acts to assist the hip in terms of stability and function.
- Used as a functional replacement for those who have undergone a hip disarticulation or trans-pelvic amputation
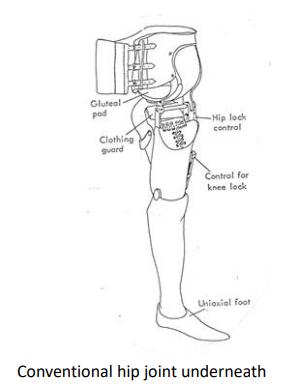
No Changes for Half a Century!
1% to 2% of amputee population
Conventional Hip Disarticulation
1954 – Canadian Hip Disarticulation – McLaurin
2008 – Otto Bock Helix Hip 7E10
2014 – Otto Bock 7E9 (Baby Helix)
Hip Joints


Knees
Types
Locked
Free
Single axis and polycentric
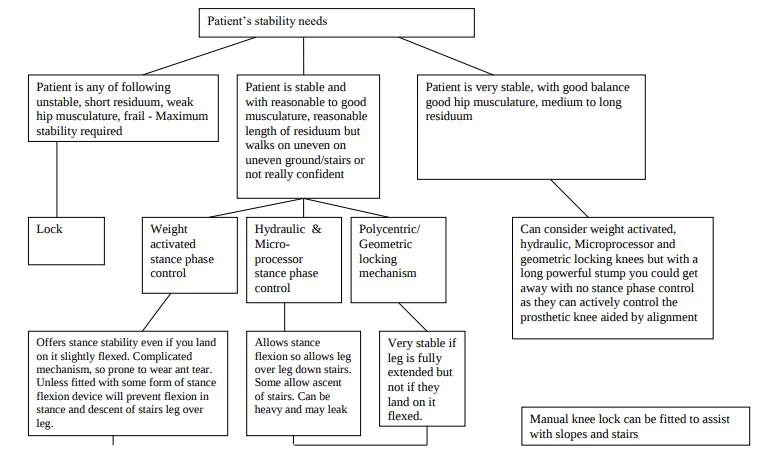
Stance phase controls – alignment, polycentric, weight activated friction brake, Hydraulics and MPK (hydraulic and magnetorheological)
Swing phase controls – friction, pneumatic, hydraulic, extension assist and MPKs
Knee Prescription - Stability
Knee Prescription - Swing
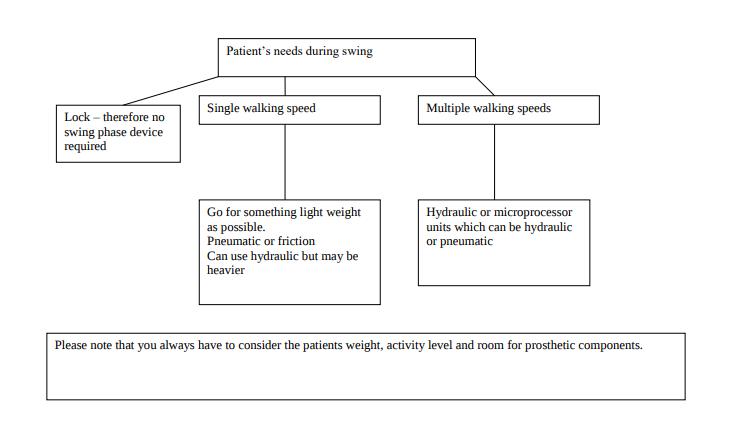
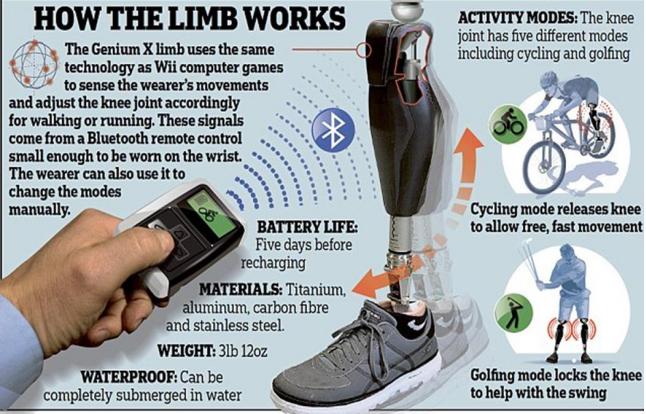
Key prescription options: Micro Processor Knees (MPK’s)mark>
Feet
Types
SACH (Solid Ankle Cushioned Heel)
Single axis
Multi-axial
Running
Energy storing / response –Can also be have ground compliance
Auto-adaptive –microprocessor ankles
Hydraulic ankles
Height adjustable
Factors Affecting Children
Cause of limb absence and its impact – Congenital/trauma/illness
When do we start rehabilitation?
Available componentry
Amputation type – retention of growth plates, end bearing
Bony growths
Changes in height
Body image/self esteem
The Parents
Funding for sports prosthesis (2016 further announcement 2018)
Cosmesis
- Body image
- Changes in attitude to cosmesis
- Impact on function
- Social anxiety
Funding
Differs in different parts of UK – Postcode lottery
Murrison funding for veterans
Funding for sports prosthesis for children in England (2016 further announcement 2018)
English funding for the use of microprocessor knees (MPKs) - https://www.england.nhs.uk/wp-content/uploads/2016/12/clincomm-pol-16061P.pdf
Scottish funding - https://www.retis.scot.nhs.uk/prosthetic.html
Welsh funding for the young - http://www.govopps.co.uk/newfund-to-provide-sports-prosthetics-for-children-and-youngpeople-in-wales/
Psychology
Reaction to amputation
Factors that impact on adaptation to amputation
Compliance
Living with a chronic disease
Psychological well being and outcomes
Paralympics
Positive growth
Economics
Phantom Limb Pain
Painful feeling associated with an absent limb through amputation
Differs from phantom limb sensation which does not include pain and residual pain which is within the residuum.
Variable findings of the percentage who experience phantom limb pain
Hampers quality of life (Trevelyan, Turner, & Robinson, 2016)
Little evidence for one effective treatment (Collins, 2018)
MDT/Interdisciplinary
Improvement of general health – cardiovascular, core strength, Muscle strength, fixed flexion contractures.
Care of chronic conditions – diabetes, rheumatoid arthritis etc
Learning to use the prosthesis
MPKs – we need to train out bad habits that were previous strategies.
Outcome Measures
Examples
Prosthetic Evaluation Questionnaire – self reported quality of life and functional outcomes
Psychosocial outcomes
Socket comfort score – self reported 1 – 10 scale
Two-Minute Walk Test
Six-Minute Walk Test
Timed “Up & Go” Test
Activity monitors
Self reported falls
Hospital Anxiety and depression scale
Changes in K levels 0-4/Sigam A-F
Areas for the Future
Brain based control?
Muscle based control?
Increase in powered movement?
Increased control of individual segments?
Increased use of osseo-integration?
New manufacture techniques?
Different shape capture techniques?