Upper limb Prosthetics
Introduction
David W. Dorrance, the original designer of the “Split Hook,” in 1912 (US Patent 1042413).
- Dorrance, lost his hand in 1909 in a sawmill accident, was unhappy with the immovable single “pirate’s hook,”
- He developed the split hook which allowed items to be squeezed and held in conjunction with a harness and straps
Level and Cause of Amputation
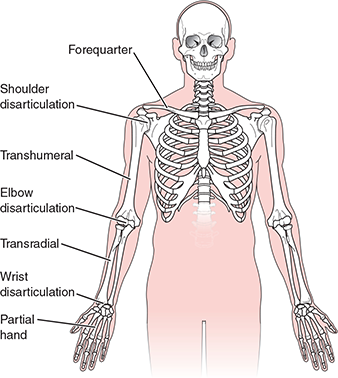
Number of referrals to UK disablement service centres in 2011⁄12 following a respective amputation at the appropriate level (bilateral in brackets):
- Forequarter: 12
- Shoulder disarticulation: 14
- Transhumeral: 95 (2)
- Elbow disarticulation: 3
- Transradial: 148 (3)
- Wrist disarticulation: 15
- Partial Hand: 70 (2)
- Loss of finger digit(s): 102 (2)
Twiste M. Limbless statistics, 2011⁄12 Available at: http://www.limbless-statistics.org/
Causes of Upper Limb Absence
- Trauma
- Congenital deficiency
- Cancer
- Infection
- Other
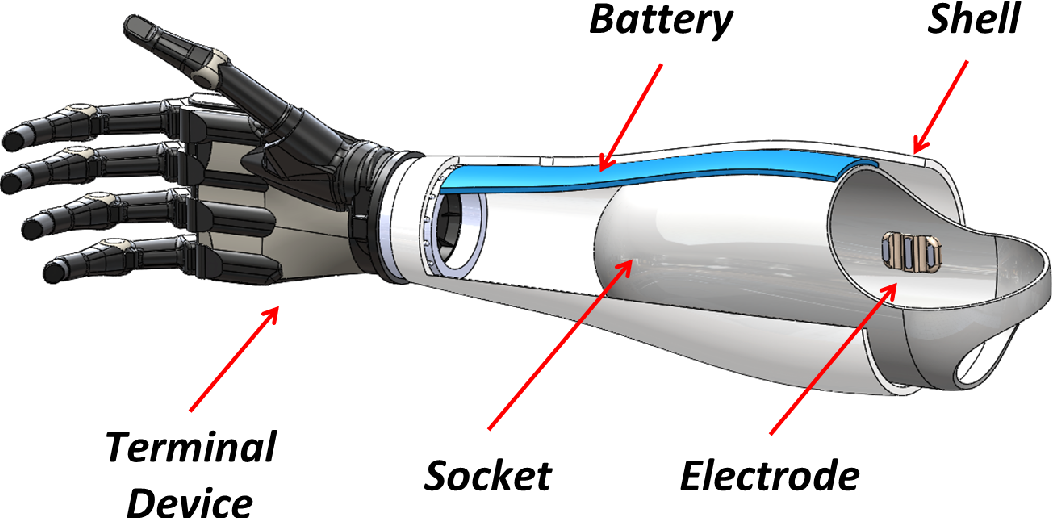
The Components of an Upper Limb Prosthesis
The socket, or prosthetic interface:
- Replacement joints, e.g. wrist, elbow
- Connecting elements
- Terminal devices, including hands
- Suspension systems, such as harnesses
- Control systems, such as myoelectric control
The Socket-Shape Capture, and Fit
Shape capture to create the correctly fitting socket usually begins with a plaster of Paris cast, that is rectified and used as a model to manufacture a prosthetic socket
Sockets are often contoured around existing bony anatomy, and can thereby suspend the prosthesis without any other form of external suspension system
Sometimes however this isn’t possible, or desired

Roll-on sockets
Developed by Ossur Kristinsson in the 1980’s, culminating in his paper
Prosthetics and Orthotics International, 1993, 17, 49-55. The ICEROSS concept: a discussion of a philosophy. Ö. Kristinsson.
ICElandic Roll On Silicone Socket (ICEROSS)
Employs ‘quasi hydrostatic’ suspension mechanism
Other Suspension Options

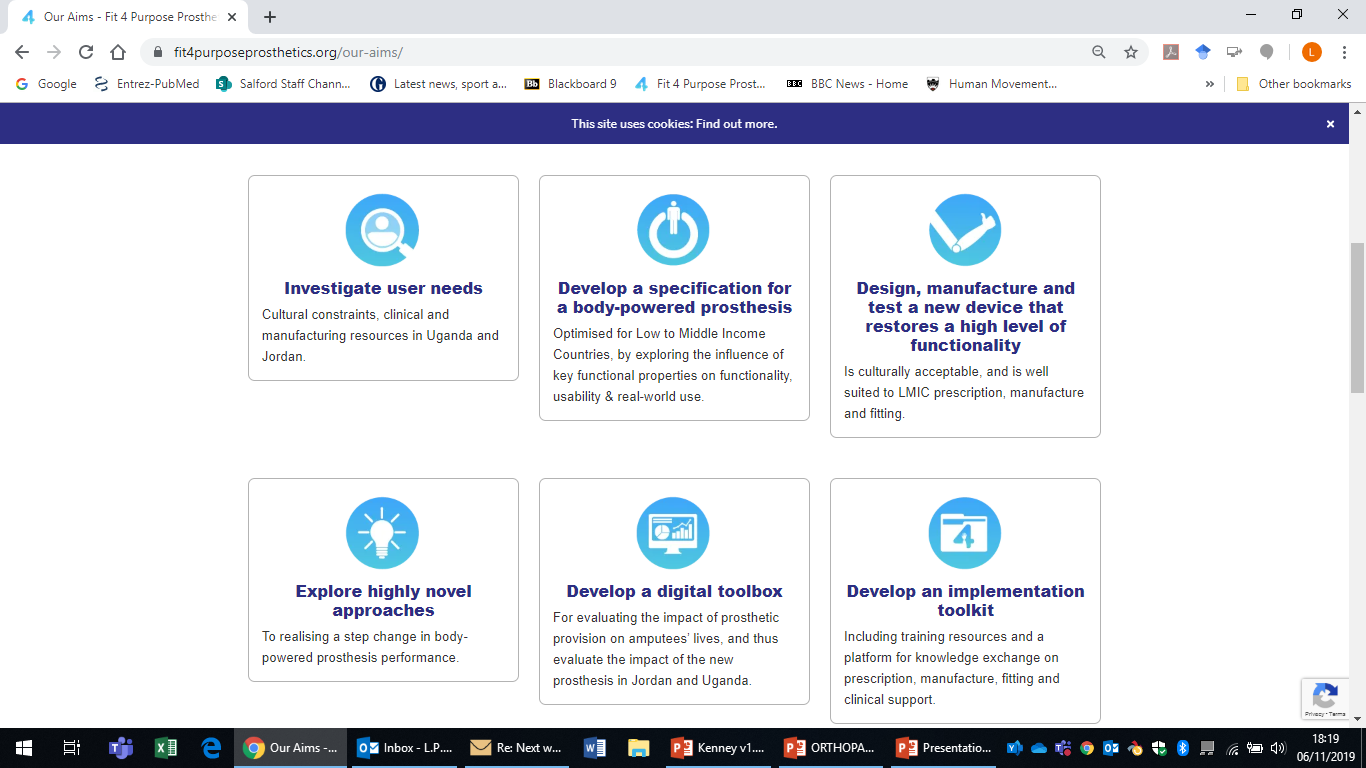
Fit 4 Purpose Prostheses
Upper Limb Functionality and Control: A Challenge to Reproduce
The natural upper limb is a complex tool, that is used to perform a wide variety of functions
From activities of daily living, to communication, social use and cultural applications, the natural hand and the arm has a wise range of functional and other applications which makes it very difficult to replicate
Types of Modern Prostheses
- Cosmetic prostheses
- Body powered prostheses
- Myoelectric prostheses
Cosmetic Prostheses
Designed to replicate the cosmetic size, shape and appearance of the missing limb, these can also act as basic holding or securing tools
They are the most commonly prescribed upper limb prostheses
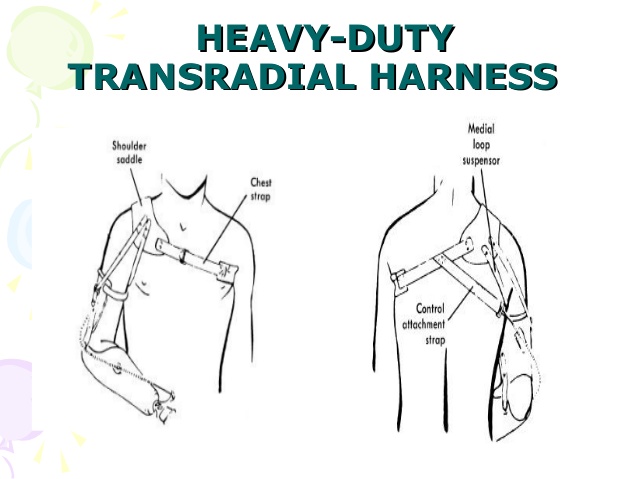
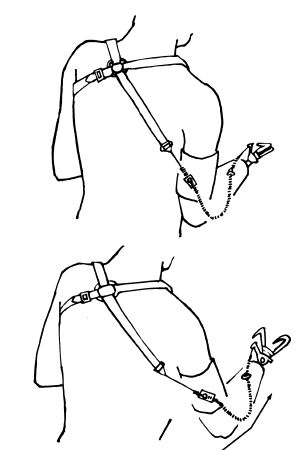
Body-powered Prostheses
Uses a biomechanical harness: either a:
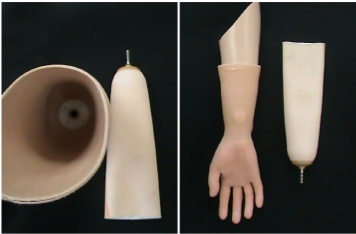
Full appendage - used to suspend and operate the terminal device in conjunction with a ‘cup’ socket, or a:
Simpler harness such as a P-loop (transradial only), which will only be used to operate the terminal device and will be used with a self suspending socket
Advantages: Good feedback, good control
Disadvantages: Poor cosmesis, dated design, comfort of harness
May be either active (with prehension) or passive (no prehension)
- Passive e.g. foam hands, knife appliance
- Active e.g. split hooks
- May be interchangeable when used in conjunction with single knob wrist rotary

Myoelectric Prostheses
Advantages over body powered devices:
- More powerful, greater grip strength and opening
- No need for harness for control
- Can potentially use limb in more positions around the body
- High-tec appeal
- Open to improvements in technology
Disadvantages:
- Heavy, costly, not as durable, harder to control, usually slower, less proprioception (feedback)
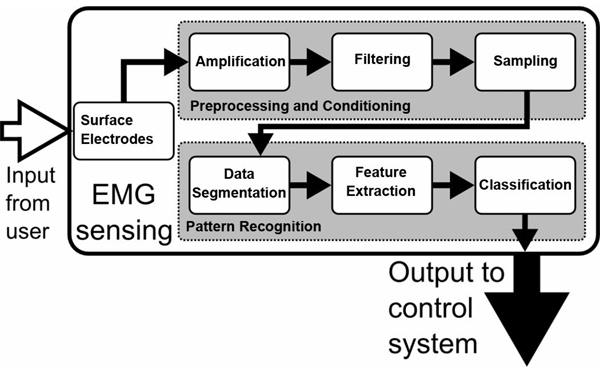
Myoelectric Signals
Created when muscles contract, these provide means of operating electrically powered prostheses
They are picked up and amplified via electrodes located within the inner wall of the socket
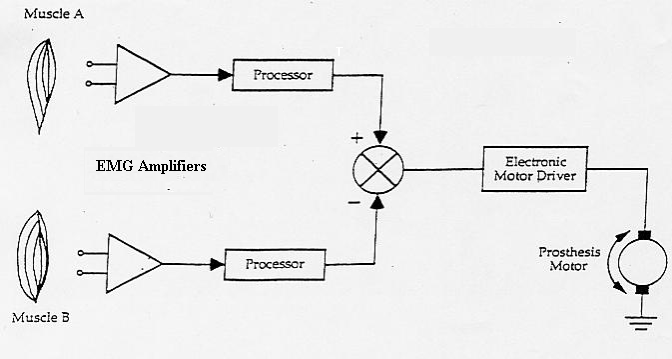
Myoelectric Control System
Types of Myoelectric Control
Threshold: 15 microvolts at skin’s surface; any signal above this = same response from hand
Proportional: 15 microvolts required for action again, but stronger signal=equivalent proportional response from the hand or component
Site/State: no. of electrodes used= no. of sites no. of functions = no. of states
Most hands are single degree of freedom hands, offering one grip type only
Multi-Functional Hands
- 14 grip patterns
- passive wrist options including low profile
- Full hand grip, individual motors in each finger and thumb

- 7 grip patterns
- Independently controlled thumb option
- Thumb, forefinger and middle finger grip
- Axon electric wrist option
The Clinical Reality
Real-world Usage:
Chadwell A, Kenney L, Granat MH, Thies S, Head J, Galpin A, Baker R, Kulkarni J. Upper limb activity in myoelectric prosthesis users is biased towards the intact limb and appears unrelated to goal-directed task performance. Scientific reports. 2018 Jul 23; 8(1):11084.
Actual Control
Head, J.S., Howard, D., Hutchins, S.W., Kenney, L., Heath, G.H. and Aksenov, A.Y., 2016. The use of an adjustable electrode housing unit to compare electrode alignment and contact variation with myoelectric prosthesis functionality: A pilot study. Prosthetics and orthotics international, 40(1), pp.123-128.
Current Challenges To Achieving Better Myoelectric Control
- Socket-related movement artefacts
- Size and clarity of signal
- Number of available control ‘modes’
Socket related movement artefacts: common mode voltage and its effects
The human body acts like a giant antenna, and attracts electricity from sources such as overhead power cables, the mains supply and electrical appliances
As a result, it constantly carries a ‘common mode voltage’ many times larger than a myoelectric signal
If the electrode is displaced in relation to the skin’s surface, then a movement artefact, very similar in size and strength to the myoelectric signal, will be produced
Filtering the signal
The common mode voltage is filtered using a differential amplifier.
As the contracting signal is discharged along the length of the muscle, the difference at each myode is registered as a positive and a negative signal and the difference is amplified
If the electrode moves or lifts, the common mode voltage may become active, or a small electrical signal may be caused by the electrode and the skin acting as charged capacitors
Size and Clarity of the Signal: Cross-Talk
Cross talk occurs when a muscle other than the target muscle affects the signal acquisition
Often occurs in congenital cases, where standard muscle boundaries are less well defined
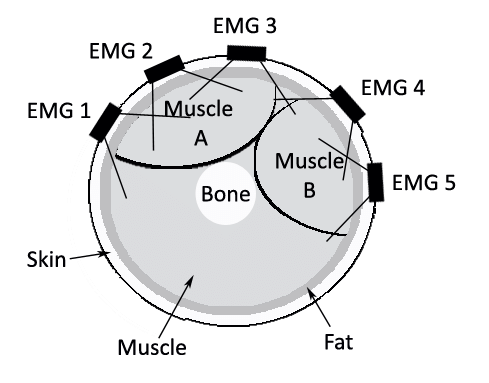
Subcutaneous Fat & Surface Impedance
Subcutaneous fat will increase the chance of cross talk and dissipate the signal, reducing its strength at the surface
Surface impedance caused by skin particles, hairs and other barriers will also affect signal size and clarity
Kuiken, T.A., Lowery, M.M. and Stoykov, N.S., 2003. The effect of subcutaneous fat on myoelectric signal amplitude and cross-talk. Prosthetics and orthotics international, 27(1), pp.48-54.
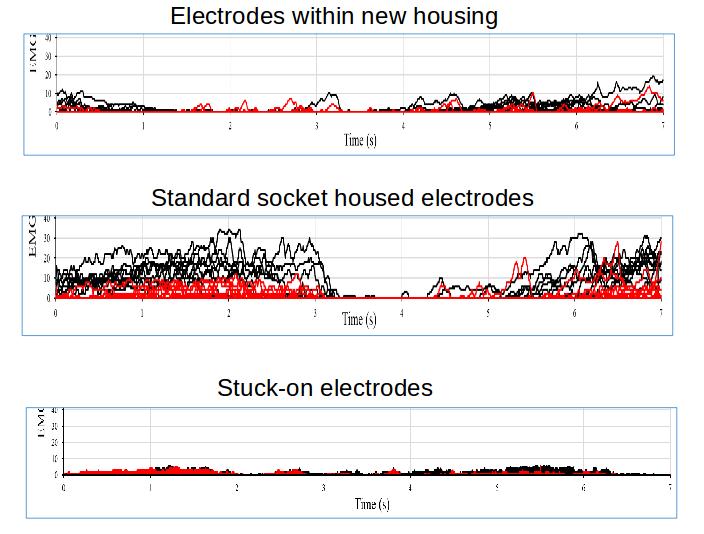
Potential Solutions: Adjustable Electrode Housing, with De-coupling from the Socket
Use of an adjustable housing with de-coupling has produced an 83% reduction in signal production above prosthesis ‘activation’ thresholds during simple arm movements
Options to Improve Control Modes
Pattern Recognition
Englehart, K. and Hudgins, B., 2003. A robust, real-time control scheme for multifunction myoelectric control. IEEE transactions on biomedical engineering, 50(7), pp.848-854.
Targeted Muscle Re-ennervation
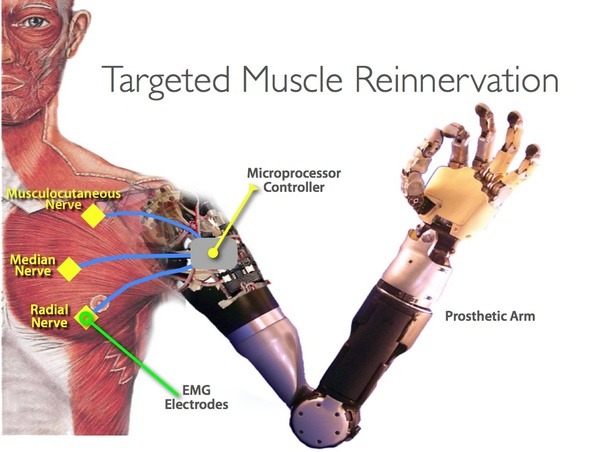
Kuiken, T.A., Li, G., Lock, B.A., Lipschutz, R.D., Miller, L.A., Stubblefield, K.A. and Englehart, K.B., 2009. Targeted muscle reinnervation for real-time myoelectric control of multifunction artificial arms. Jama, 301(6), pp.619-628.
Kuiken, T.A., Dumanian, G.A., Lipschutz, R.D., Miller, L.A. and Stubblefield, K.A., 2004. The use of targeted muscle reinnervation for improved myoelectric prosthesis control in a bilateral shoulder disarticulation amputee. Prosthetics and orthotics international, 28(3), pp.245-253.
Summary
Despite recent advances, we still have along way to go to improve upper limb prostheses, and particularly myoelectric control
Some options, such as simpler body-powered devices, would be of more benefit, particularly in developing countries and for sports and other activities
There are a number of factors that contribute to the prescription of the most suitable device, but these can be best reached with a sound understanding of each patients wishes, and requirements